


 />i
/>iIntroduction
In recent years, a number of codes on the Medicare Physician Fee Schedule have experienced significant reductions in their payment rates due to changes to a single direct practice expense input. We conducted an analysis in May and August 2018, following the publication of the CY 2019 Proposed Rule, to determine how many other codes are vulnerable to potentially significant payment reductions because their rate is tied predominantly to a single input. Our analysis found 366 codes that have the majority of their payment rate tied to a single direct practice expense input.
Helpful Resources:
-
CY 2019 Medicare Physician Fee Schedule Proposed Rule Direct PE Input
-
CY 2019 Proposed Rule Market-Based Supply and Equipment Pricing Update
-
McDermottPlus Tool to Replicate Practice Expense RVU Calculation
Background
The Centers for Medicare and Medicaid Services (CMS) and the American Medical Association Specialty Society Relative Value Scale Update Committee (RUC) are reviewing HCPCS codes on an annual basis to determine whether the code has the appropriate relative value unit (RVU) on the Medicare Physician Fee Schedule (MPFS). These reviews may be initiated based on different triggers, including the following:
-
Creation of a new code or revision to an existing procedure code in a code family
-
Periodic review of procedure codes (not less frequently than every five years) as required by Section 1848(c)(2)(B) of the Act
-
Nomination of a procedure code as part of the annual review of potentially misvalued codes, which may fall into a number of categories, including but not limited to the following:
-
Codes that have experienced substantial changes in practice expenses
-
Codes with high intra-service work per unit of time
-
Codes with high practice expense RVUs
-
Codes with high cost supplies
In conducting its review of the HCPCS codes, the RUC—on its own or at the request of CMS—is specifically seeking to determine the appropriate work, practice expense and malpractice RVUs. The practice expense RVUs, which represent 50 percent or more of the total non-facility RVUs in more than 53 percent of the codes[1], are calculated in part based on the following direct practice expense inputs.
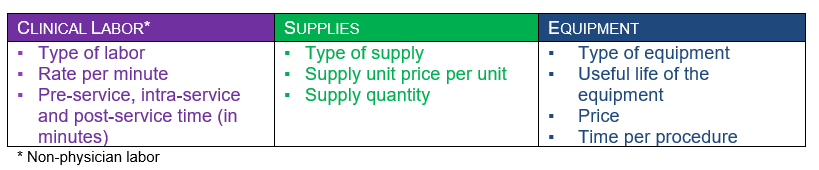
As part of the RUC process and/or the CMS review process, the units and prices are determined for the above types of inputs based on various sources. It is important to understand the specific inputs for an individual code and the relative importance of each clinical labor, supply and equipment input in determining the value for codes of interest. Substantial changes in a single input can have a dramatic effect on the overall payment rate for a code. Two recent examples in prior rulemaking cycles illustrate the impact.
Prothrombin-Time/International Normalized Ratio Home Monitoring
Home international normalized ratio (INR) monitoring has two technical components that are the key components of the service: demonstration/training (under G0248) and ongoing monitoring (under G0249).[2] In October 2015, the RUC recommended that these codes be referred to the CPT Editorial Panel for the creation of Category I codes. The Level II HCPCS “G” codes had been created to implement the National Coverage Determination in 2002, but these codes never “graduated” to Level I CPT codes or underwent RUC review of their valuations. For CY 2018, the CPT Editorial Panel created the two new codes applicable to the demonstration and training and professional interpretation of home PT/INR monitoring and for the technical component of the ongoing furnishing of testing equipment and services.[3][4] While the RUC recommended the deletion of the G codes, CMS decided to keep the existing three G codes given their use under a National Coverage Determination for home PT/INR monitoring.
While choosing to maintain the G codes, in the CY 2018 annual rulemaking cycle, CMS implemented a change in the unit price for a key direct practice expense input—INR test strips (SJ055). Specifically, CMS repriced the unit price of INR test strips from $21.86 to $5.66, a reduction of more than 74 percent. As proposed, this change in a single input would have dropped the payment rates for G0248 and G0249 by 44.2 percent and 43.4 percent when fully implemented (holding the conversion factor constant). Based on feedback from stakeholders, CMS increased the number of units for the INR test strips from four to six for G0249. With this change, the reduction of payment was mitigated by approximately 20 percent.[5]
Flow Cytometry
Flow cytometry is reported by two separate codes: one for the first marker (88184) and a separate code for each additional marker (88185).[6] In the CY 2016 annual rulemaking cycle, CMS proposed and finalized significant changes to the technical component for the two flow cytometry codes.
Specifically, CMS changed the number of units for the lysing agent (SL089) from 14 mL to 5 mL and 2 mL for 88184 and 88185 respectively. This change, as fully implemented and holding the CY 2016 conversion factor constant, would have translated into a 39.3 percent and 69.5 percent drop respectively for 88184 and 88185. In the two years since the change, a number of stakeholders have worked through the RUC process to mitigate the rate reductions by 29 percent in 88184 and 14 percent in 88185.[7]However, even with those changes, 88184 experienced a 28 percent drop, and 88185 (fully implemented and holding the CY 2018 conversion factor constant) would experience a 59.9 percent drop.[8]
StrategyGen Analysis
In the CY 2019 MPFS Proposed Rule, CMS proposed significant changes to prices for a number of direct practice expense items. These changes were based on an in-depth analysis of supply and equipment pricing conducted by StrategyGen, a market research firm that CMS engaged under its authority granted by Section 220(a) of the Protecting Access to Medicare Act. To determine “market” prices for the supply and equipment inputs under review, the StrategyGen team employed numerous approaches, including field surveys, aggregate databases, vendor resources, market scans and market analysis. Based on its analysis, StrategyGen recommended changes to almost 1,400 inputs as demonstrated in the table below.
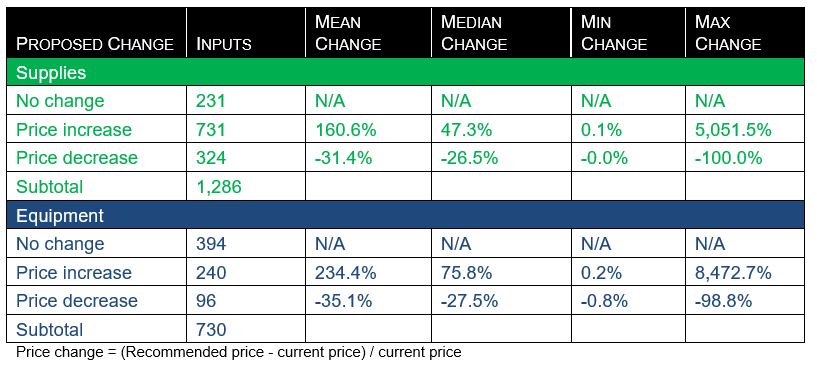
In the Proposed Rule, CMS proposed to accept all the changes, noting that while some inputs experienced changes in their prices, the overall changes were budget neutral. To account for significant changes in the proposed prices, CMS proposed to phase-in the changes to price inputs (if finalized) over a four-year period.
Vulnerable Code Analysis
Given these two recent experiences, as well as the proposed new price inputs based on the StrategyGen analysis, McDermott+Consulting conducted a detailed analysis of the direct practice expense database that CMS released with the CY 2019 MPFS Proposed Rule. The analysis focused on the non-facility setting and identified potentially vulnerable codes whose practice expense RVUs (and thus corresponding payment rates) rested in large part on a single input.
To identify potentially vulnerable codes, the following initial code-level criteria were set:
-
Non-facility PE RVU > 50 percent of total non-facility RVU
-
Volume for the code > 1,000 based on CY 2016 utilization data crosswalked to 2018 codes
-
Total cost of the input > $24.99
Then, the analysis focused on inputs at the code level within each of the three categories: labor, supply and equipment. For each category, the following two additional criteria were established:
-
Cost for the single input (at the code level) > 60 percent of total cost in that category for that code
-
Category (g., equipment, supply or labor) > 60 percent of total inputs for that code
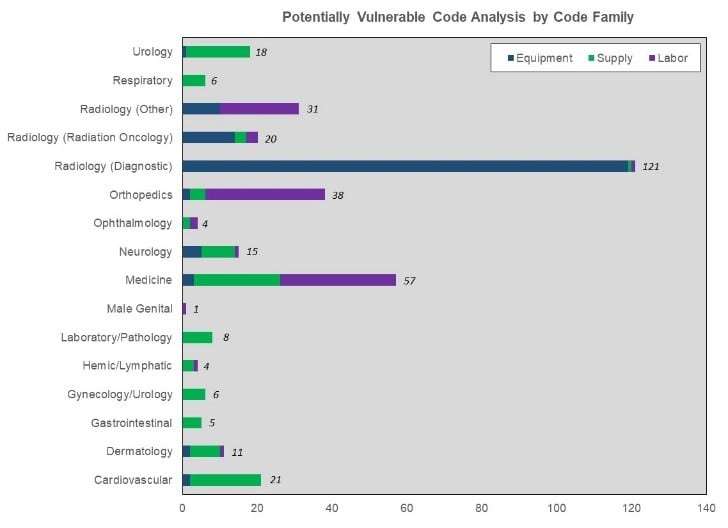
The analysis identified more than 360 codes that are potentially vulnerable based on the criteria established above. Specifically, 43.2 percent of the codes have the majority of their RVU tied to a single equipment input, with 31.1 percent and 25.7 percent of codes having the majority of their RVU tied to a single labor or supply input, respectively.
In an examination of the code family level, the 158 codes identified as vulnerable due to a single equipment input are for 11 different equipment items. This may not be surprising, as the majority are radiology codes affected by one of six items.
For the codes affected by a single labor input, the majority of the codes are either orthopedic procedures (20000 series) or medicine services and procedures (90000 series).
The three code series with the highest number of codes affected by a single supply input are cardiovascular (33010–37999), medicine (90000 series) and urology (50000–53899).
Next Steps
It is important for stakeholders to become more knowledgeable about the potentially vulnerable codes; to understand the potential impact of changes to the price, units or time for the key practice expense inputs; and to consider strategies to address these issues as appropriate.
[1] Based on codes in Addendum B of the CY 2018 MPFS Final rule where the total non-facility RVU is greater than zero.
[2] G0248 (Demonstration, prior to initiation of home INR monitoring, for patient with either mechanical heart valve(s), chronic atrial fibrillation or venous thromboembolism who meets Medicare coverage criteria, under the direction of a physician, includes: face-to-face demonstration of use and care of the INR monitor, obtaining at least one blood sample, provision of instructions for reporting home INR test results, and documentation of patient ability to perform testing and report results) and G0249 (Provision of test materials and equipment for home INR monitoring of patient with either mechanical heart valve(s), chronic atrial fibrillation or venous thromboembolism who meets Medicare coverage criteria; includes provision of materials for use in the home and reporting of test results to physician; testing not occurring more frequently than once a week; testing materials, billing units of service include four tests).
[3] 93792 (Patient/caregiver training for initiation of home INR monitoring under the direction of a physician or other qualified health care professional, face-to-face, including use and care of the INR monitor, obtaining blood sample, instructions for reporting home INR test results, and documentation of patient’s/caregiver’s ability to perform testing and report results).
[4] 93793 (Anticoagulant management for a patient taking warfarin, must include review and interpretation of a new home, office or lab INR test result, patient instructions, dosage adjustment (as needed) and scheduling of additional test(s), when performed).
[5] Assuming no other changes to the codes, these changes will be fully implemented by CY 2020.
[6] 88184 (Flow cytometry, cell surface, cytoplasmic or nuclear marker, technical component only; first marker) and 88185 (Flow cytometry, cell surface, cytoplasmic or nuclear marker, technical component only; each additional marker (List separately in addition to code for first marker)).
[7] In CY 2018, CMS finalized an increase in the number of units of antibodies per test from 1.0 to 1.6.
[8] Changes for 88185—based on the phase-in policy—are currently to be fully implemented in CY 2022.